A 62-year old healthy male had a fall from 5 feet height landing on his dominant right hand. He sustained a communuted distal radius fracture (Fig. 2).
It was a closed injury and was initially treated with manipulation under regional anaesthesia (MUA) and application of plaster cast (POP). The fracture was, however, unstable and reduction was lost at 1-week post-op.
The situation was discussed with patient and it was agreed that further attempt at fracture reduction will be undertaken. Patient was given the choice of fracture stabilisation with open reduction and internal fixation (ORIF) with plate osteosynthesis or treatment with PolyArmour Non-invasive dynamic wrist fixator.
Owing to potential benefits of avoiding open surgery, shorter hospital stay, ability to shower and bathe with the PolyArmour fixator in situ, this patient opted for the PolyArmour Non-invasive dynamic Wrist fixator (Fig.1).
The procedure was carried out as day-case with application of PolyArmour Non-invasive Wrist fixator and manipulation under anaesthesia (Fig. 3a & b). An anatomical reduction was achieved with optimal stabilisation.
The device was set in a rigid mode for 2 weeks. Check radiographs at 2 weeks were satisfactory and range of motion (ROM) from 0⁰ Dosi-flexion to 30⁰ Volar-flexion was commenced. This was increased to 15⁰ Dosi-flexion and 45⁰ Volar-flexion at 4 weeks (Fig. 4a & b).
Free ROM was instituted in Dorsal-Volar plane at 5 weeks. The fixator was removed at 6 weeks and the clinical assessment showed that the patient immediately had 75⁰ Dorsi-flexion, 75⁰ Volar-flexion and complete pronation-supination.
No Physical therapy was needed. Radiographic assessment at 2, 4, 6, 9 and 12 weeks show no displacement of fracture and optimal healing and patient achieved complete and pain free range of motion.
Patient reported satisfactory comfort, easy to maintain his lifestyle, light weight device and degree of movement early on in his treatment as the principal advantages for him. Patient reported outcome was ‘excellent’.

Fig. 1: PolyArmour Non-invasive wrist fixator on a patient with a right distal radius fracture.

Fig. 2: Right distal radius fracture.
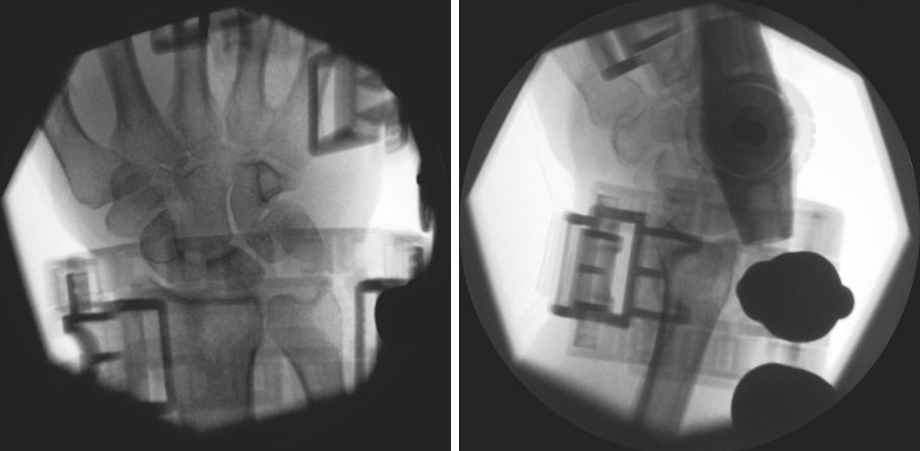
Fig. 3 a & b: Application of PolyArmour Non-invasive Wrist fixator with anatomical reduction of fracture.

Fig. 4 a & b: Four weeks post-op with PolyArmour Non-invasive wrist fixator in-situ allowing selective motion at the wrist joint.

Fig. 5: Anatomically healed fracture in patient treated with PolyArmour Non-invasive Wrist fixator who has an excellent functional result.